Every death from suicide is a tragedy. But research shows that its rates can be reduced with greater understanding and support.
To do this, suicide should be recognised as a public health problem, and people should know that it can be prevented and its rates can be reduced.
On this page we show data on the prevalence of suicide across the world, its risk factors, and how these trends are changing over time.
If you are dealing with suicidal thoughts you can receive immediate help by visiting resources such as findahelpline.com.
Key insights on Suicide data & research
Suicide rates vary around the world
Suicide rates vary widely between countries. The map shows this.
For some countries in Southern Africa and Eastern Europe, the estimated rates of suicide are high, with over 15 annual deaths per 100,000 people.
Meanwhile for other countries in Europe, South America and Asia, the estimated rates of suicide are lower, with under 10 annual deaths per 100,000 people.
The wide range in suicide rates around the world is likely the result of many factors. This includes differences in underlying mental health and treatment, personal and financial stress, restrictions on the means of suicide, recognition and awareness of suicide, and other factors.1
What you should know about this data
- Suicide estimates come from death certificate data, using deaths that were classified under death codes for ‘intentional self-harm’ in the International Classification of Diseases (ICD). This includes people who had self-harmed but had not intended to die, and they may not be considered suicides by the country’s particular legal definition.
- In many countries, deaths due to self-harm are highly underreported due to social stigma, cultural and legal concerns. Instead, these deaths are often misclassified in reported data, especially as deaths due to “events of undetermined intent”, accidents, homicides, or unknown causes. To account for this, the WHO’s Global Health Observatory reclassifies a proportion of deaths reported with those causes as suicides, according to the fraction that are estimated to be deaths by suicide. As a result, data on suicide rates represent a better estimate of how many people die from suicide.
- Suicides may still be underestimated after this adjustment, especially if they are misclassified as other types of deaths.2 This can also be why some countries appear to have rising suicide rates, if the rates of misclassification decline.

Suicide rates have declined in many countries
In many countries, suicide rates have declined substantially.
You can see this in the chart, which shows the change since the year 2000. It shows estimates for countries in Europe that surpass an indicator for data quality on suicides. These include Spain, Italy, Norway, Austria, Luxembourg, Finland and France.
These large declines in suicide rates have been partly driven by greater awareness and help for people at risk, improvements in mental health treatment, and restrictions on some of the methods of suicide.3
This tells us that suicide is preventable. But many countries don’t take enough action to drive down its rates. Suicide may not be tackled effectively, or may not even be seen as a public health concern.4
What you should know about this data
- It’s possible to get an indicator of data quality on suicides by looking at the ratio of unexpected deaths to suicides. If there is a lower ratio of unexpected deaths to suicides, this implies that a higher proportion of unexpected deaths were classified as suicides, which is an indicator of better data quality. In the chart we show a selection of countries in Europe where suicide rates have declined and which had a low ratio of unexpected deaths to suicides, as identified by Värnik and colleagues (2012), which implies that they had higher quality data on suicides. This included Spain, Italy, Norway, Austria, Luxembourg, Finland and France.5 Several of these countries also have very high rates of validation by coroner reports, and/or have autopsies performed for almost all unexpected or injury deaths.6
- Suicide estimates come from death certificate data, using deaths that were classified under death codes for ‘intentional self-harm’ in the International Classification of Diseases (ICD). This includes people who had self-harmed but had not intended to die, and they may not be considered suicides by the country’s particular legal definition.
- In many countries, deaths due to self-harm are highly underreported due to social stigma, cultural and legal concerns. Instead, these deaths are often misclassified in reported data, especially as deaths due to “events of undetermined intent”, accidents, homicides, or unknown causes. To account for this, the WHO’s Global Health Observatory reclassifies a proportion of deaths reported with those causes as suicides, according to the fraction that are estimated to be deaths by suicide. As a result, data on suicide rates represent a better estimate of how many people die from suicide.

Deaths by suicide are under-reported in many countries
In many countries, suicides are under-reported for a number of reasons. A major reason is that deaths in general – not just suicides – are not well-recorded in many countries. You can see this in the chart.
It shows that in some cases, not all deaths are registered in a country’s central vital registration system. In many countries, especially in Africa and South Asia, a low share of deaths are registered in such systems at all.
Where vital registration systems are underdeveloped, statisticians have to estimate the number of deaths and their causes from partial data and particular studies.
Researchers typically define suicides as deaths which were classified as deaths caused by ‘intentional self-harm’ in the International Classification for Diseases (ICD). This includes people who had self-harmed but had not intended to die, and they may not be considered suicides by the country’s particular legal definition.
Self-harm deaths tend to be under-recorded, even among countries that have a large share of deaths registered.7
This is partly because, in many countries, suicide is highly stigmatised. In some countries, suicides and suicide attempts can be a criminal offence.8 For these reasons, suicides may be misclassified, especially as deaths due to “events of undetermined intent”, accidents, homicides or unknown causes.9
To account for this, the WHO and IHME reclassify a proportion of deaths reported with those causes as suicides. This is done according to the fraction that are estimated to be deaths by suicide. As a result, data on suicide rates represent a better estimate of how many people die from suicide, but they may still be underestimated after this adjustment, especially if they are misclassified as other types of deaths.10
What you should know about this data
- This comes from the International Completeness of Death Registration dataset, developed by Ariel Karlinsky.11
- The total number of expected deaths per year is an average of estimates from three data sources – the UN’s World Population Prospects, WHO’s Global Health Estimates and IHME’s Global Burden of Disease study.
- For many countries, their estimates are very similar. However, for others, where vital registration systems are lacking or not functional, they tend to differ.
- The level of death registration may also vary widely across different regions within these countries.12

Suicides are more common among men
Across countries, the estimates show that suicide rates are much higher among men than women.
This is shown in the scatterplot, which compares estimates of suicide rates among women (on the horizontal axis) to the rates among men (on the vertical axis).
Almost all countries are located above the gray diagonal line, which means that the suicide rate was higher among men than women.
But the size of the gender disparity varies widely between countries. Some countries lie close to the line, meaning they have a smaller gender disparity. Other countries lie far away and have a large gender difference.
What you should know about this data
- Suicide estimates come from death certificate data, using deaths that were classified under death codes for ‘intentional self-harm’ in the International Classification of Diseases (ICD). This includes people who had self-harmed but had not intended to die, and they may not be considered suicides by the country’s particular legal definition.
- In many countries, deaths due to self-harm are highly underreported due to social stigma, cultural and legal concerns. Instead, these deaths are often misclassified in reported data, especially as deaths due to “events of undetermined intent”, accidents, homicides, or unknown causes. To account for this, the WHO’s Global Health Observatory reclassifies a proportion of deaths reported with those causes as suicides, according to the fraction that are estimated to be deaths by suicide. As a result, data on suicide rates represent a better estimate of how many people die from suicide.
- Suicides may still be underestimated after this adjustment, especially if they are misclassified as other types of deaths.13 This can also be why some countries appear to have rising suicide rates, if the rates of misclassification decline.

Mental illnesses are a major risk factor for suicide
There are many risk factors for suicide, including bullying, financial distress, and trauma.14
A large risk factor is mental illness, especially if it is not treated. On average, people who are diagnosed with a mental illness tend to have a higher risk of suicide.
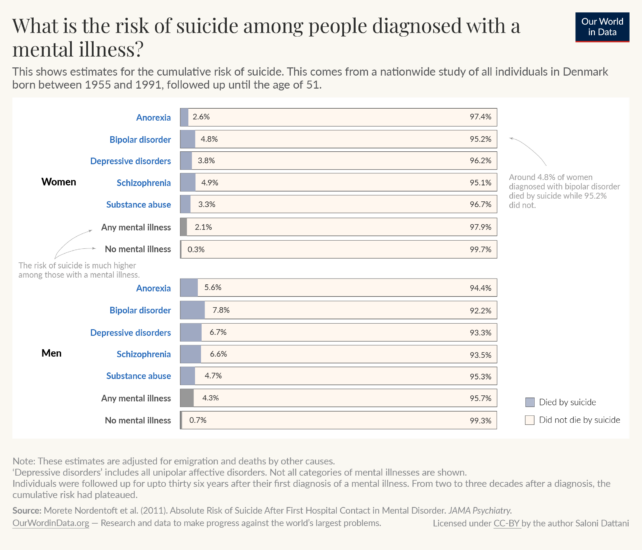
The chart shows estimates of the risk of suicide from a nationwide study in Denmark, using data from the entire population aged between 15 and 51.
Around 2.1% of women and 4.3% of men who were diagnosed with a mental illness died by suicide, versus 0.3% of women and 0.7% of men without a mental illness.
Importantly, the chart also shows that the vast majority of people – with or without a mental illness – did not die by suicide. Even among those diagnosed with a mental illness, the risk of suicide can be reduced substantially with treatment.15
What you should know about this data
- This study uses data from the entire population of Denmark until the end of 2006.16 Since the study was published, the cumulative risk of suicide may have changed.
- The data included all diagnoses made in in-patient psychiatric hospitals and, from 1995 onwards, all out-patient clinics. The large sample size allows for precise estimates of the risks of suicide and how they relate to clinical diagnoses.
Suicide rates may vary with age
In some countries, such as the United States and Japan, you can see that suicide rates tend to be similar across age groups.
However, in some other countries, such as South Korea and Portugal, you can see that suicide rates tend to be higher among older age groups.
That suicide rates can be much higher among older people may sound surprising, because suicide is a leading cause of death in young people. But it is because deaths due to other causes tend to rise with age at a much faster rate than deaths by suicide.
The rates of death from other causes such as cardiovascular disease, cancers, dementia, and respiratory diseases, rise steeply with age throughout the lifespan.
However, the rates of deaths from suicides, accidents, and other ‘external causes’ tend to rise steeply from childhood until adulthood.17 After this, some countries show a continued rise in suicides with age, while others do not.18
Differences between countries are likely to result from many factors, just as there are differences in the overall rates of suicide around the world. For example, they may result from differences in underlying mental health and treatment, personal and financial stress, restrictions on the means of suicide, recognition and awareness of suicide, and from changes over generations.19
What you should know about this data
- Suicide estimates come from death certificate data, using deaths that were classified under death codes for ‘intentional self-harm’ in the International Classification of Diseases (ICD). This includes people who had self-harmed but had not intended to die, and they may not be considered suicides by the country’s particular legal definition.
- In many countries, deaths due to self-harm are highly underreported due to social stigma, cultural and legal concerns. Instead, these deaths are often misclassified in reported data, especially as deaths due to “events of undetermined intent”, accidents, homicides, or unknown causes. To account for this, the WHO’s Global Health Observatory reclassifies a proportion of deaths reported with those causes as suicides, according to the fraction that are estimated to be deaths by suicide. As a result, data on suicide rates represent a better estimate of how many people die from suicide.
- Suicides may still be underestimated after this adjustment, especially if they are misclassified as other types of deaths.20 This can also be why some countries appear to have rising suicide rates, if the rates of misclassification decline.

Interactive charts on Suicides
 Number of suicidesWHO data
Number of suicidesWHO data Suicide rateWHO data, age-standardized
Suicide rateWHO data, age-standardized Suicide rate, by ageWHO data
Suicide rate, by ageWHO data Suicide rates among young people
Suicide rates among young people Male vs. female suicide rateWHO data
Male vs. female suicide rateWHO data Male vs. female suicide rateIHME data
Male vs. female suicide rateIHME data Male-to-female ratio of suicide rateIHME data
Male-to-female ratio of suicide rateIHME data Male-to-female ratio of suicide rateWHO data
Male-to-female ratio of suicide rateWHO data Number of suicide from firearms
Number of suicide from firearms Number of suicide from pesticide poisoning
Number of suicide from pesticide poisoning Number of suicidesIHME data
Number of suicidesIHME data Number of suicides, by ageIHME data, since 1990
Number of suicides, by ageIHME data, since 1990 Share of deaths from suicide
Share of deaths from suicide Share of suicides from pesticide poisoning
Share of suicides from pesticide poisoning Suicide death rateIHME data
Suicide death rateIHME data Suicide rateIHME data, age-standardized
Suicide rateIHME data, age-standardized Suicide rateWHO data
Suicide rateWHO data Suicide rate by firearm
Suicide rate by firearm Suicide rate in 1990 vs. 2019IHME data
Suicide rate in 1990 vs. 2019IHME data Suicide rate in 2000 vs. 2019WHO data
Suicide rate in 2000 vs. 2019WHO data Suicide rate vs. death rate from violenceIHME
Suicide rate vs. death rate from violenceIHME Suicide rate vs. depressive disorders rate
Suicide rate vs. depressive disorders rate Suicide rate vs. homicide rateWHO; UNODC
Suicide rate vs. homicide rateWHO; UNODC Suicide rate vs. income inequality
Suicide rate vs. income inequality Suicide rate vs. prevalence of mental & substance use disorders
Suicide rate vs. prevalence of mental & substance use disorders Suicide rate, by ageIHME data
Suicide rate, by ageIHME data Suicide rate, by age
Suicide rate, by age Suicide rate, by sexWHO data
Suicide rate, by sexWHO data