Seasonal flu is a contagious illness caused by the influenza virus. It kills around 400,000 people from respiratory disease on average each year. In large pandemics, when new strains have evolved, the death toll has been much higher.
Yet, data on the flu is limited. With better testing, countries could improve their response to flu epidemics. It could help to rapidly identify new strains, detect epidemics early, and design better-matched vaccines to target flu strains circulating in the population.
This page therefore shows estimates of deaths during seasonal flu epidemics, historical flu pandemics, patterns of flu seasons in different countries, and confirmed cases of flu and flu-like symptoms across the world.
It also includes our Flu Explorer, a resource for epidemiologists, infectious disease researchers, and public health experts to monitor the global spread of the influenza virus.
Key insights on Influenza
Seasonal flu kills hundreds of thousands of people worldwide each year
The flu is estimated to cause 400,000 respiratory deaths each year on average across the world. These deaths come from pneumonia and other respiratory symptoms caused by the flu.1
People also die from other complications of the flu – such as a stroke or heart attack – but global estimates have not been made of their death toll.2
The flu is most severe in infants and the elderly.3
Among those over 65, the flu kills around 31 people per 100,000 each year from respiratory disease in Europe. You can see this on the map.
But it’s not only age that matters, as the map shows. Death rates from the flu are higher in countries in South America, Africa, and South Asia, than in Europe and North America, due to poverty, poorer underlying health, lower access to healthcare, and lower vaccination rates.
In this article, we provide more detail:

What you should know about this data
- The annual mortality rate of influenza was estimated by the Global Pandemic Mortality Project II using data between 2002 and 2011.4 They made these estimates using data from routine surveillance metrics for the flu, along with the number of excess deaths that occurred during flu seasons and mortality records where deceased people had respiratory symptoms.
- These are estimates of flu deaths due to respiratory symptoms. People also die from other complications of the flu – such as a stroke or heart attack – which are not included here.
- Estimates in low-income countries tend to be less certain due to lower levels of testing for influenza and limited mortality records.

Seasonal flu used to be far more deadly
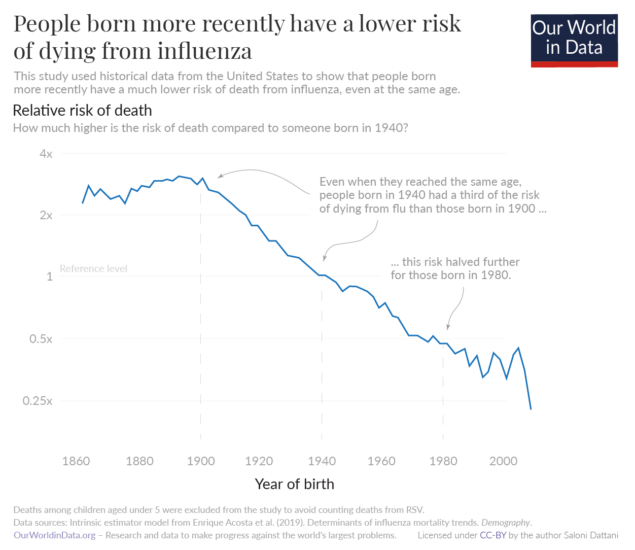
Over time, the severity of the flu has declined among people of the same age, as the chart shows.11
This is because of flu vaccination, which began in the 1930s and 1940s, as well as improvements in sanitation, neonatal healthcare, and childhood vaccination for other diseases.12 These benefits carried forward as people aged: they protected people from being vulnerable to diseases including influenza.
But the flu still causes a large burden today, especially in countries that have poor sanitation, healthcare, and low vaccination rates.
Another challenge is that populations have been aging rapidly.13 In lower-income countries, the flu could become a larger burden as their populations continue to age.
In this article, we provide more detail:
What you should know about this data
- These estimates come from a study by Enrique Acosta and colleagues, using data from the United States.14
- The authors use national data on deaths and routine surveillance data for flu to calculate the rate of excess deaths during flu seasons, while accounting for changes in the age structure of the population.
- The chart shows that the risk that someone dies from influenza at a given age has declined over time. But, because the population is getting larger and older, the total number of flu deaths has remained stable.
The Spanish flu caused the largest influenza pandemic in history
Some flu seasons are far more severe than usual seasonal influenza.
This happens when influenza viruses combine with each other to make new strains which are more infectious and lethal, and lead to deadly pandemics.32
For example, the Spanish flu pandemic was caused by a combination of human influenza and another animal influenza. Together, they formed the new H1N1 virus.33
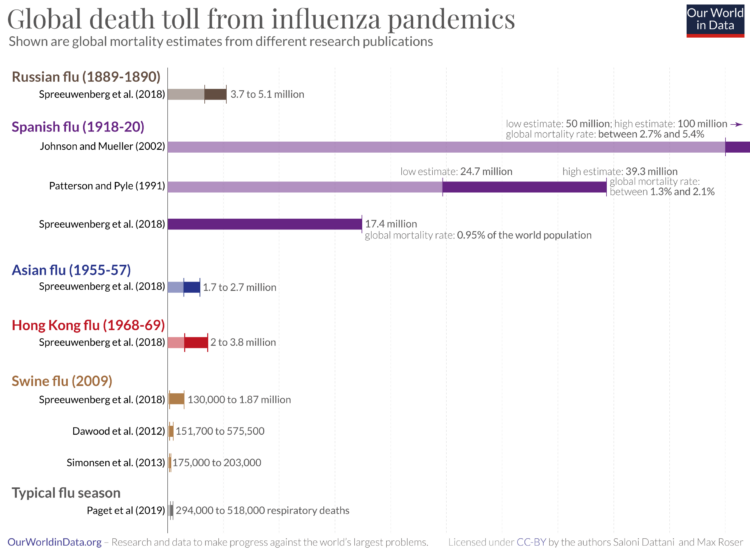
As you can see in the chart, it led to the most devastating influenza pandemic in recorded history. Estimates of the death toll vary: some studies estimate that 17.4 million people died globally from the Spanish flu between 1918 and 1920, while others estimate a much higher death toll of 50 to 100 million deaths.34
The Spanish flu pandemic was most severe among children and young adults. Life expectancy at birth and at young ages declined by more than ten years.
But surprisingly, it did not have a significant impact on older people. Research suggests that this is because older generations had been exposed to similar H1 influenza viruses decades before the pandemic began, which gave them some protection against the Spanish flu strain.35
In this article, we provide more detail:
What you should know about this data
- In the chart, we show a comparison of mortality estimates from different research groups for recent flu pandemics in history.36
- Estimates for historical flu pandemics tend to come from data on mortality rates. Pandemics cause sudden shocks to mortality compared to typical years. Researchers can calculate the excess mortality during the pandemic to estimate the deaths they caused while adjusting for other known factors, such as famine and war.
- There are still large uncertainties in each estimate, because historical mortality records are limited in many countries. However, the range of estimates for these pandemics is much higher than a typical flu season. For the Spanish flu pandemic, estimates are more than an order of magnitude higher.
Explore our data on influenza
Why we provide this Influenza Data Explorer
With this Flu Explorer, we aim to provide a helpful resource for epidemiologists, infectious disease researchers, and public health experts to understand the global spread of the influenza virus.
It differs from our widely-used infectious diseases projects, such as the COVID-19 Explorer and the Mpox Explorer. These tools are designed for a broad audience. Unfortunately, flu data is incomplete in many ways, making it harder to communicate. This tool is therefore designed for users with pre-existing knowledge to navigate effectively the complex data published by the World Health Organization.
The explorer also highlights the significant gaps in influenza data. It is an important reminder of the need to improve data collection and reporting.